Restricting drugs no cure for costs?


{jcomments on} On June 10th, Geraldine Vance, the chief executive officer of the British Columbia Pharmacy Assocation, wrote an Oped in the Vancouver Sun titled "Restricting drugs no cure for costs". The article below is a rebuttal.
On June 10th, Geraldine Vance, the chief executive officer of the British Columbia Pharmacy Assocation, wrote an Oped in the Vancouver Sun titled "Restricting drugs no cure for costs". The article below is a rebuttal.
On June 10th, Geraldine Vance, the chief executive officer of the British Columbia Pharmacy Assocation, wrote an Oped in the Vancouver Sun titled "Restricting drugs no cure for costs". The article below is a rebuttal.Vance paints a rather simplistic and one-sided story regarding the (rising) costs of health care and the cost of prescription medication in particular.
Her key point was that although New Zealand may have reduced spending on pharmaceuticals that may not be the way we should go. Vance cites as reasons that the New Zealand approach restricts choice, that it is a complex issue, and that there may be negative health and cost effects. The problem is that Vance does not substantiate any of her opinions and while I appreciate Vance for starting this important discussion I think a bit (actually a lot) of context is needed.
Those are the opinion pages (in the Vancouver Sun), however we cannot have a good discussion without facts and data.
Since Vance uses New Zealand as an example of how we maybe not should try to reduce spending costs, let’s have a look some key facts on Canada and New Zealand. How much do we spend on pharmaceuticals and Health Care?
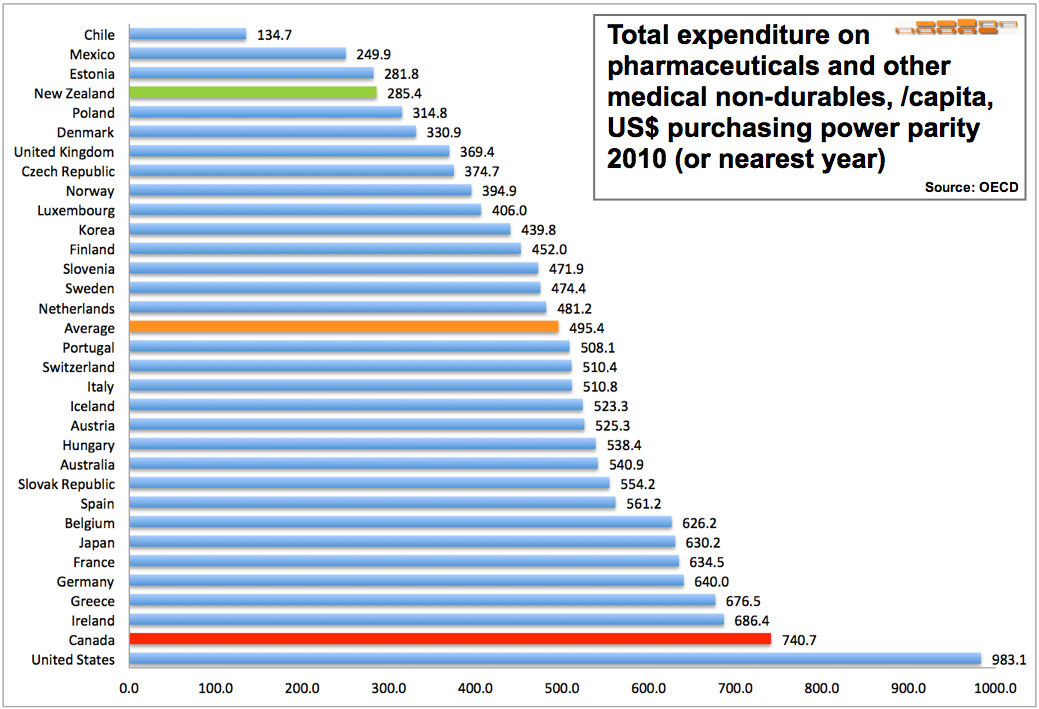
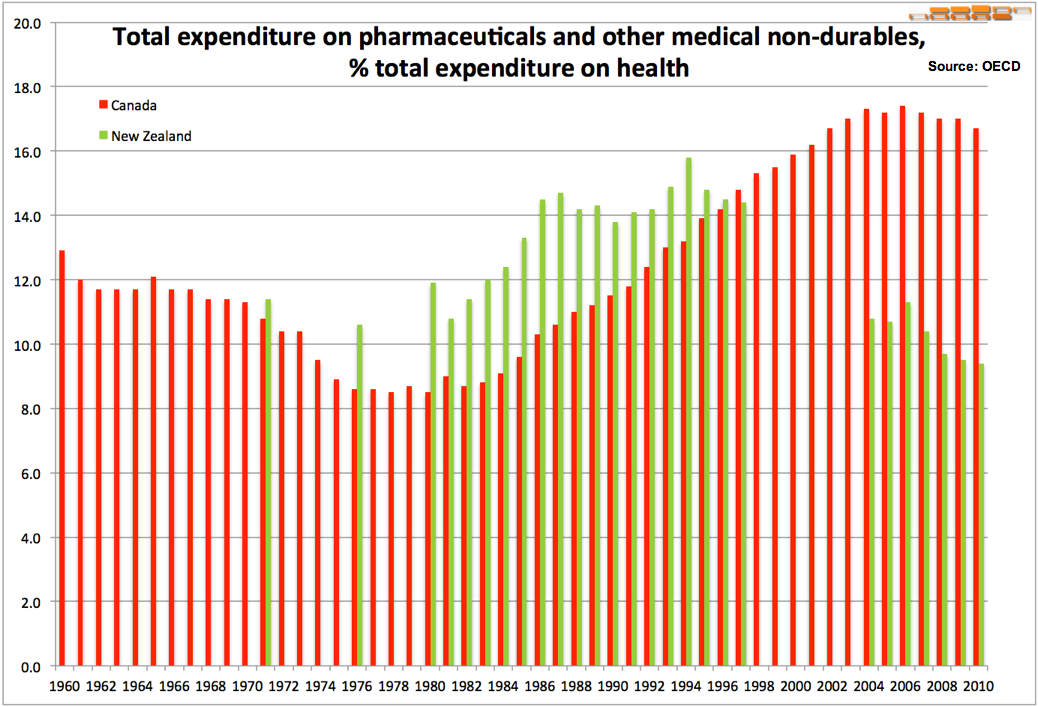
The total expenditure on pharmaceuticals and other medical non-durables, per capita in US$ purchasing power parity in 2010, provided by the OECD , for Canada was $740.7. For New Zealand it was $285.4 and the average for all OECD covered countries was $494.5.
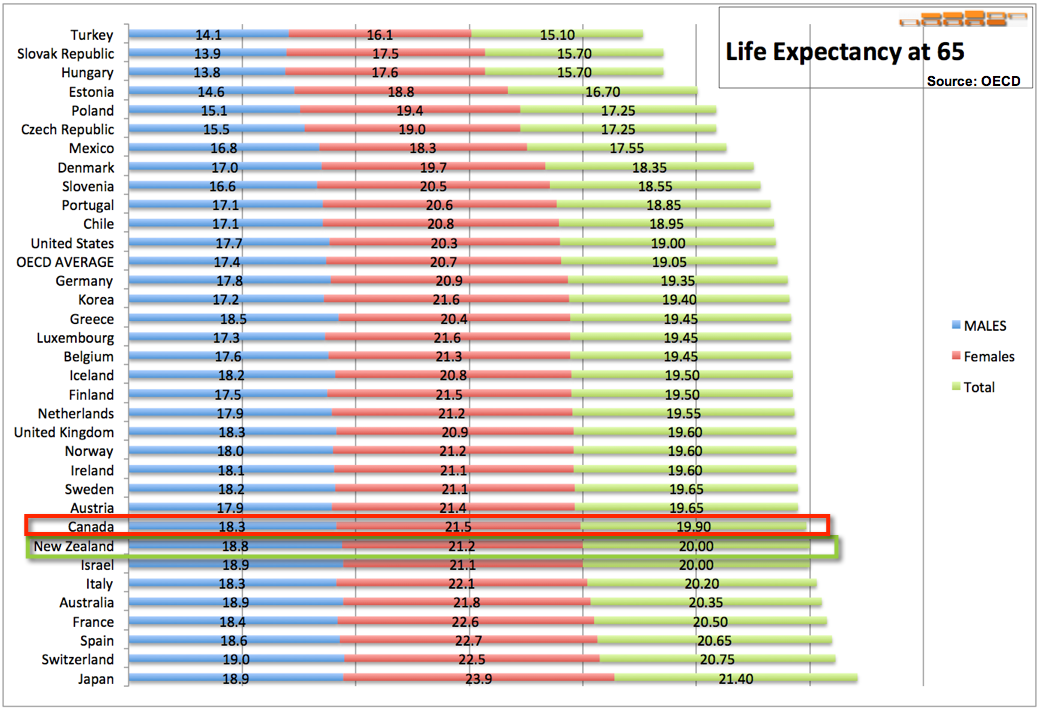
Looking at how much countries spend per capita on health care without looking at health outcomes is kind of useless. Since Vance mentions the aging populations let’s have a look at how Canada and New Zealand compare for “Life Expectancy at age 65”. In other words, for people who are currently 65, how many more years can they expect to life, on average of course. For Canada the numbers for 2010, are, 18.3, 21.5 and 19.9 respectively for males, females and the total population. For New Zealand the numbers are 18.8, 21.2 and 20.
And finally let’s have a look at the perceived quality of health. The last year for which data is available for both countries is 2007. The percentage of the population, aged 65 years old and over who report their health to be 'good' or 'better', was, in 2007, 74.5% and 83.2% for Canada and New Zealand respectively.
In other words while spending only just over a third of what Canada spends on medications life expectancy and perceived quality of health is higher in New Zealand. I am the first to admit that there are many factors that influence these factors but it makes one think when Vance says: “The way to control the total cost of drugs and deliver best health care results is with a comprehensive approach to patient care, not just one that counts the pennies of drug costs”. Maybe pinching pennies has given New Zealand the budgetary room to improve the health care system elsewhere. Who knows?
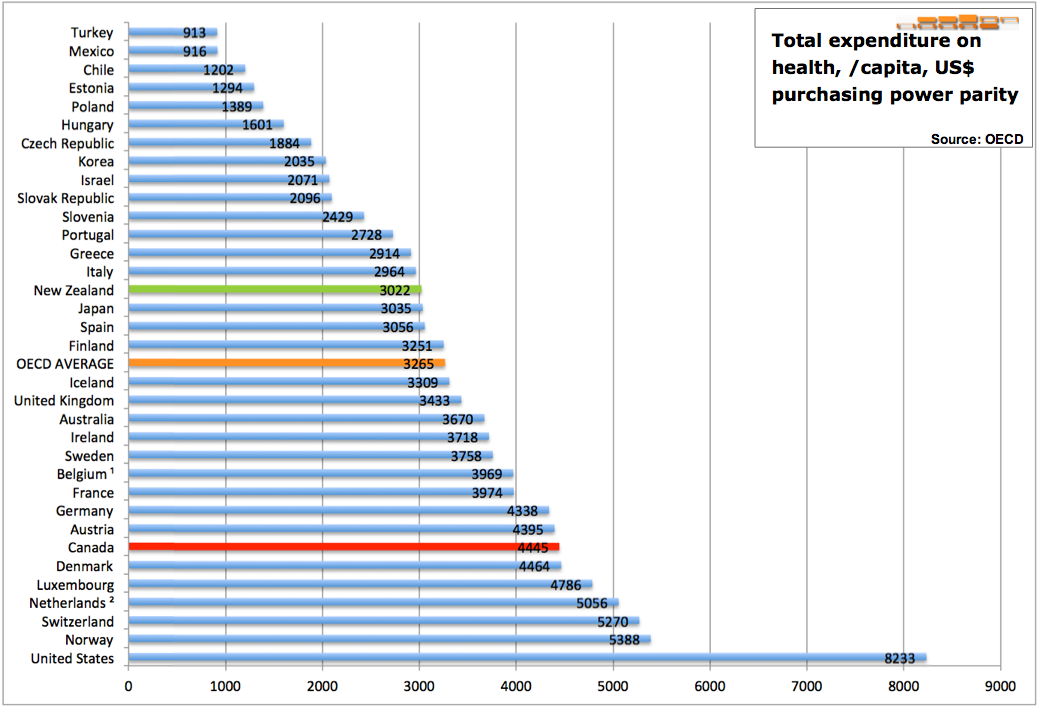
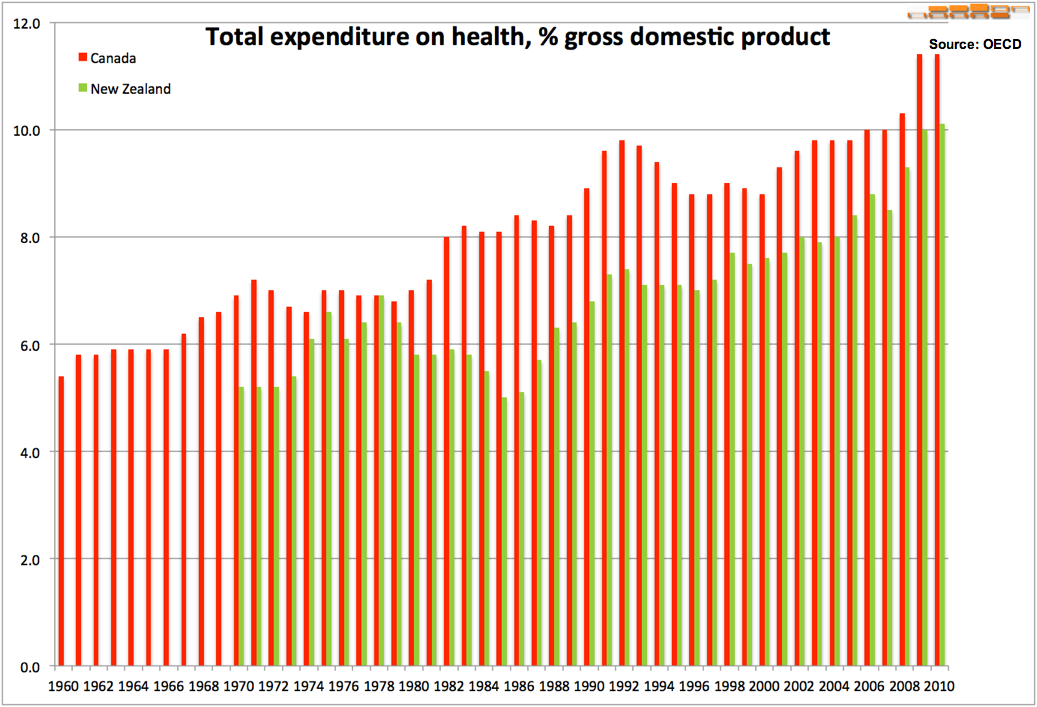
Since Vance tries to make the point that withholding choice of medications and non compliance of medication may have a negative cost effect on the health care system it is only fair to look at the total health care spending for both countries. On a per capita basis Canada spends $4445 and New Zealand $3022. The OECD average is $3265.
Secondly I will comment on a few statements Vance makes.
In the 5th paragraph states that the restrictions imposed on patients, physicians and pharmacists in New Zealand, most British Columbians would find unacceptable. She never explains why. Surely if you posit it as a limitation of freedom without looking at the benefits of the restrictions most people in BC would oppose it. If on the other hand you explain the why, the how and the what, including hard data the people in BC might not oppose it.
Next Vance states that the range of medications available to patients is severely restricted. However, she does not explain a) which medications and b) whether that is good or bad. By putting it this way Vance implies this is a bad thing. She never explains why.
Paragraph 8 is again a great example of this style of arguing, that is, without evidence and based on instilling negative images. I totally agree that if cost management gets in the way of patient focused care that would be a problem. The issue I have is the way in which Vance makes that statement. Vance implies this is what is currently happening in New Zealand. She does not provide one iota of evidence cost management gets in the way.
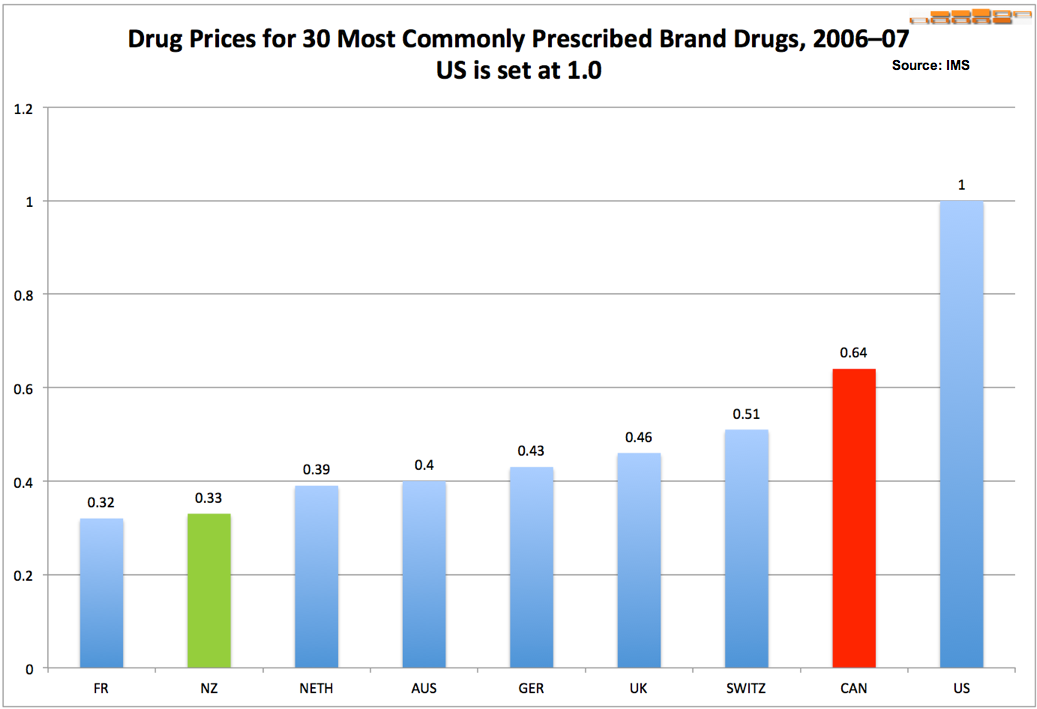
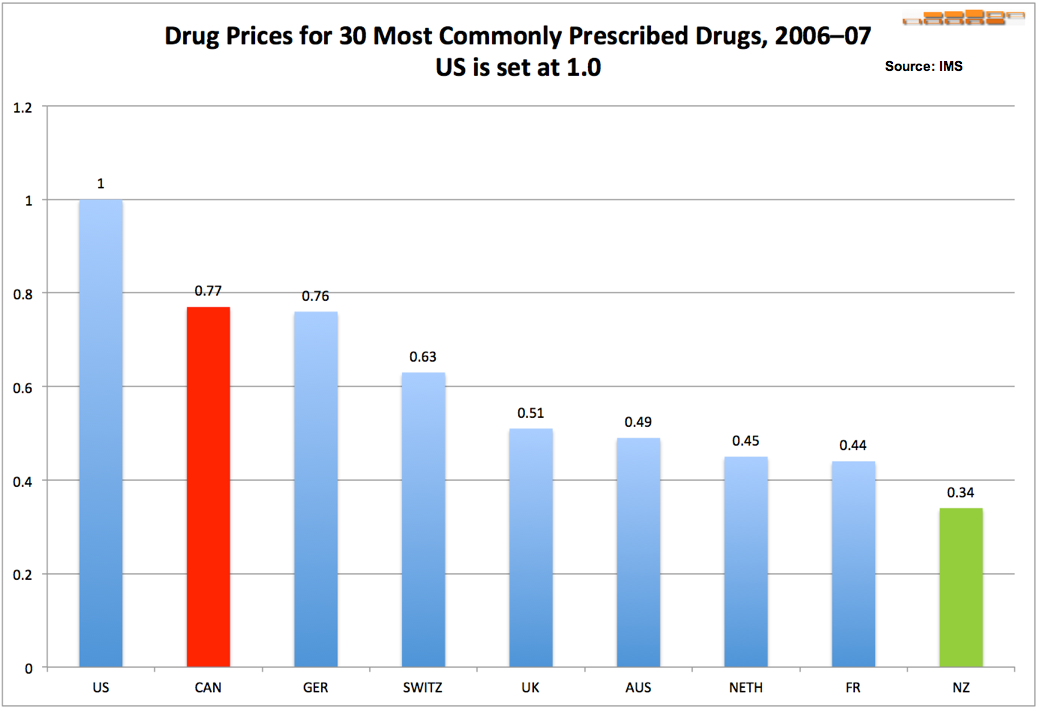
It may be true that one of the contributors to the rising PharmaCare budget is the growth in the volume of prescriptions as Vance sates in the following paragraph. However, Vance fails to mention that the prices we pay in Canada for medications are much higher than in New Zealand as one can see below.

Paragraphs 12 and 13 are troublesome as they contain a, what I would call, you can’t have it both ways fallacy. Vance argues that medication non-compliance comes at a great cost. She first names comprised health as a cost factor and then mentions the cost of the wasted medications as a factor of those cost. However, those medication costs are not incremental. They are so called sunk cost. The reason being that if there would be no non-compliance those medications would still cost the same!
The next two paragraphs (14,15) deal with the changing role of Pharmac. I argue that the information Vance provides is minimalist at best. In 1998 Pharmac already ran a campaign aimed at the inappropriate use of antibiotics. In 2010 the NZ government released a report suggesting indeed a wider role for Pharmac. This widening however is not only focused on giving Pharmac a bigger role in medication management but also to adopt the Pharmac model for medical devices! It is unfair to imply that the approach of New Zealand, as per the last sentence of paragraph 15, is solely based on penny counting.
In her concluding paragraph Vance once more uses the term 'simplistic' thus implying not 'thoroughly thought through'. The prescription in itself is indeed simple. Control cost by having a national/provincial procurement strategy. Implementation is of course far from simplistic. Finally Vance ties all this back to limiting choice again without explaining why that would not be a good idea. She certainly did not prove that not restricting choice is better.
Finally it is important to not only look at absolute numbers - since they will always rise given the growth in GDP and inflation - but to also look at cost as a percentage of GDP and all health costs. Again New Zealand outperforms Canada. Not only that, it appears spending on drugs in Canada seems to slow down. As a matter of fact, that is also something the Canadian Institute for Health Information (CIHI) reports. Lots to think and talk about.
In closing I want to address the inevitable retort I expect. Do I have a better solution for our increasing? No I do not have a silver bullet at my disposition. I have some ideas, such as the Pharmac approach, giving prescribers better access to medication costs, patient drug profiles and access to medication educational material to name a few.
I agree this is a complex issues that requires a comprehensive approach. With comprehensive we must also mean making sure all the available data is used and reviewed. No cherry picking please.
Erik Hamburger
Sources:
OECD for country statistics
Multinational Comparisons of Health Systems Data, 2010 by Common Wealth Fund.
Canadian Institute for Health Information (CIHI) for detailed information
Welcome



... your FuTuRe ...
We established Ambidexter Management as a concept and go-to place for people who want to effectively manage their business and life.
Get great material
Learn from others
Share your successes
...It's free!
Login or Sign-up now

Let us lend you a helping hand. We are Ambidexter after all!
